HISTORY:
E. rhusiopathiae was isolated by Koch in 1878 and described by Pasteur and Thuillier in 1882 as the bacteria responsible for the red swine disease, communicable disease against which they prepare a live attenuated vaccine.Rosenbach in 1884, has been isolated in humans, from skin lesions, a bacterium identified as that described by Pasteur and Thuillier. The human disease has been described by Baker in the end of the century. The development of anti-mullet serum and vaccines in 1891 with virulent or attenuated live bacteria were, before the era of antibiotics, highly effective means of struggle against the disease in animals (especially pork) .
I – GENERAL CHARACTERISTICS OF GENRE:
 E. rhusiopathiae is the only species of the genusErysipelothrix This is a fine bacillus, straight or slightly curved, variable in size. 0.2-0.4 x 2.5 [im down to either “short “but may be in the form of long filaments of several tens of microns. Non-spore forming bacteria are not encapsulated, motionless, Gram-positive, facultative anaerobic and negative aero-for catalase and oxidase tests. They have low fermentation activity.
E. rhusiopathiae is the only species of the genusErysipelothrix This is a fine bacillus, straight or slightly curved, variable in size. 0.2-0.4 x 2.5 [im down to either “short “but may be in the form of long filaments of several tens of microns. Non-spore forming bacteria are not encapsulated, motionless, Gram-positive, facultative anaerobic and negative aero-for catalase and oxidase tests. They have low fermentation activity.
This genetically homogeneous type (G + C Ploo between 36-38) is one of Gram-positive bacteria nonsporulated regular shape like other genera Lactobacillus, Listeria,which may be encountered in humans.
II – HABITAT AND EPIDEMIOLOGY:
E. rhusiopathiae is a ubiquitous bacterium widely distributed in nature.
It can be isolated from mammals, birds and fish. Pigs (30 to 50% of healthy carriers) is probably the species most commonly affected (swine erysipelas), but diseases may also reach other animals, domestic and wild mammals, breeding birds. In fish, the bacteria can be isolated from the mucus covering the surface of the body, but does not cause infection.
The bacterium is present in water and soil where it seems to persist for several years, remarkable performance for a non-spore-forming bacterium and made a “telluric” bacteria. Similarly, the bacterium persists for several years in dead animals and several months in the smoke and salt meat.
Human contamination occurs after contact with infected animals. The disease is primarily professional when handling animals or carcasses of pigs, poultry, fish, and therefore observed in veterinarians, butchers, slaughterhouse workers, but also farmers and fishermen. The skin entrance, on the hands is the most common. Oral and gastrointestinal entrance doors are much rarer.
III – PATHOGENICITY NATURAL:
E. rhusiopathiae is the agent of swine erysipelas, acute septicemic disease with cutaneous and articular manifestations or subacute and chronic with locations in the endocardium and joints.
In humans, the most common form is localized cutaneous form erysipeloid Baker and Rosenbach. After a short incubation period of 2-3 days, the site of inoculation (small wound, excoriation) is the seat of an erythematous area, warm, sensitive, itchy, giving an impression of power and burns. This zone extends gradually, giving a red placard vinous, slightly raised, but clearer and collapsed in the center, surrounded by a peripheral bead purple. The localized injury to the hand can involve the entire dorsum of the hand and is accompanied by axillary lymph nodes and épitrochléennes. There has never suppuration and spontaneous healing can be observed in a few weeks.
The septicemic forms are rare, occurring immediately or after a cutaneous form. They are most often associated with endocarditis or septic arthritis occur in susceptible individuals. Other locations (pulmonary, meningeal, pleural) are also rare.
Some products developed by E. rhusiopathiae may play a role in the virulence of the organism such as hyaluronidase and neuraminidase.
IV – BACTERIOLOGICAL DIAGNOSIS:
Direct diagnosis is envisaged, the indirect diagnosis with limited interest.
A – The specimens:
Blood culture is the essential collection during sepsis. In the cutaneous form, if there is a blister, we seeded the liquid; if the lesion is dry, the bacteria is located at the bead in the dermo-epidermal layers and isolation of the organism is difficult. To have the best chance to isolate the bacteria, we must take a sample with a scalpel at the bead (melon side without bleed).
The germ can also be isolated from joint fluid or CSF in humans.
In live animals, isolation is made from blood cultures. From dead animals, use of enrichment media supplemented with antibiotics or inhibitors of other bacteria.
B – Direct examination:
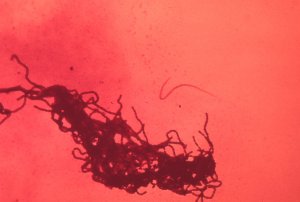
Microscopic examination is rarely positive on skin biopsy. In culture, E. rhusiopathiae is a straight or slightly curved bacilli, Gram-positive, immobile, non-encapsulated, non-spore forming. Large size variations are observed: 0.2-0.3 x 1-5) Jm in young cultures and filaments of several tens of microns in older cultures. Form long filaments, it takes the form of clumps
hair (hence part of its name: thrix).
C – Culture:
Culture is enhanced by the presence of glucose or serum and by a slightly alkaline pH. E. rhusiopathiae is optional aero-anaerobic, microaerophilic more readily during isolation.
There is an S shape and form R. The S shape corresponding short forms and gives fine colonies (1 mm in 24-48 hours), smooth, curved, shiny, transparent, edged, becoming opaque after several days. The long filaments correspond to the shape which gives R flat colonies, opaque, matt and rough surface, irregular edges (Bacillus anthracis colonies in miniature). The dissociation of colonies in both directions can be observed.
On blood agar colonies cause hemolysis sometimes intense alpha but never hemolysis beta type.
The optimum temperature for cultivation is 30-37 ° C, but culture is possible between 5 and 42 ° C.
The germ grows slowly and weakly in usual medium, its growth is promoted by the addition of blood, serum, ascites or glucose.
D – Identification – Experimental pathogenicity:
Devoid oxidase and catalase, this bacterial genus has a low metabolic activity.
Glucose and lactose were acidified without gas production; rhamnose, sucrose, mannitol and esculin are not changed. There is no production of indole in peptone water and the nitrates are not transformed.
The bacterium lacks urease occurs slowly in the middle of H2S in the lead acetate or mid-Kligler Hajna. Gelatin stab on the culture of E. rhusiopathiae gives an image characteristic pipe cleaner, without liquefaction of gelatine (22-25 ° C).
Two species, mouse and pigeon are particularly susceptible to experimental infection.
Mice injected intraperitoneally or subcutaneously with 0.1 ml of a 24 hour culture causes death in 24-48 hours. The bacterium is found in all organs (liver, spleen … and is especially visible in the kidney decals) and heart blood.
E – Differential diagnosis:
E. rhusiopathiae is a rarely encountered bacteria in routine medical bacteriology. The differential diagnosis it deserves more attention. Several species of bacilli Gram-positive non-spore forming should be considered(Corynebacterium, Lactobacillus, Listeria) and even Gram-positive cocci (Streptococcus). A table showing the main differential characteristics between these species is found in the chapter “Listeria.” The characters in take into account, in addition to the morphology and respiratory type are: catalase, oxidase, growth temperatures, the culture or not enriched environments, esculin hydrolysis, production of H2S, mobility, the acid culture medium (MRS), metabolism and glucidolytique protéoly tick.
Experimental pathogenicity in mice optionally with a protection assay by the specific antiserum can complete identification and differential diagnosis.
F – Classification – serotypes:
Specific heat labile antigens species and type of specific thermostable were identified. The specific type of polysaccharide antigens are used to define nature and 22 serotypes (serotypes). Serotypes 1 and 2 are the most frequent.
There is at least a group of antigen and, in some strains, a vaccine antigen and an HA antigen have been described.
V – TREATMENT AND PREVENTION:
Treatment consists of antibiotics; Penicillin is the antibiotic of choice. The strains are sensitive to tetracyclines, macrolides, chloramphenicol, streptomycin.
In severe cases (sepsis, endocarditis) an assocation is recommended: G / streptomycin penicillin or ampicillin / gentamicin. The treatment should be extended over a month; relapses are not uncommon.
Prophylaxis is limited to the precautions to be observed by those who, through their work are in contact with sick animals or carriers of germs or with animal products that may be contaminated with the bacterium erysipelas.
You must be logged in to post a comment.