* Tobacco: high risk beyond 20 PA; Carcinogenic: benzopyrene and polycyclic hydrocarbons; nitrosamines;phenols; arsenic.
* Other FDR: asbestos (amphibole overcoats, for little or no chrysotile); arsenic; nickel; chromium; iron oxide;hydrocarbons; beryllium; ionizing radiation.
* Genetic factors: HLA B12 group.
* Late effects of tuberculosis -> adenocarcinoma
A- General:
* Natural history: Rapid doubling time, particular clinical presentation, metastatic potential.
* Therapeutic: no surgical indication (with exceptions); but very radiosensitive and chemotherapy
* Poor prognosis, even after complete remission.
* 20% of lung cancer

B- Pathology:
* Comes from the malignant transformation of multipotent cell bronchial stump of endodermal origin, neuroendocrine differentiation (this explains the presence of tumors combined with non-small contingent adénocarcinomateuses or squamous cells).
* Central (main bronchus or lobar) submucosal extension; early lymphatic invasion; common extrathoracic extension at diagnosis.
* Metastatic sites are in descending order: liver, adrenal, bone, CNS, bone marrow.
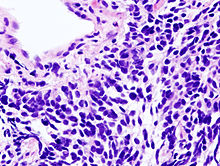
* Optical Microscopy: oat grain (or oatcell) but can be combined or intermediate (larger) (squamous or glandular contingent of cells).
* Electron microscopy: the presence of neurosecretory grains characteristics
* Markers: do not express lymphocyte markers (Dc differential with lymphoma); ADH; neuropeptides (NSE, VIP).
C- paraneoplastic syndromes endocrinological:
* Inappropriate ADH secretion (Schwartz-Bartter syndrome) involving profound hyponatremia and natriuresis retained.
* Ectopic secretion of ACTH (ACTH like) -> Cushing’s syndrome with melanodermia
* Inappropriate secretion of TRH -> hyperthyroidism
* Inappropriate secretion of insulin -> Hypoglycemia
* Inappropriate secretion of ß-HCG or prolactin -> gynecomastia
D- Paraneoplastic neurological syndromes:
* Lambert-Eaton syndrome: muscle weakness with areflexia (pseudo gravis with blocking presynaptic)
* Denny-Brown: severe sensorimotor neuropathy predominant on the upper limbs
* Other: Myelitis (Landry’s syndrome); limbic encephalitis (rapidly progressive dementia); polymyositis.
E- paraneoplastic syndromes and other skin:
* Acanthosis nigricans: mainly stomach cancer, diabetes field
* Hyperkeratosis painful palms of hands and soles of the feet (basex)
* ++ Recurrent phlebitis
F- Two paraneoplastic syndromes are more often associated with squamous cell carcinoma:
* Hypercalcemia (for secretion of PTH like hormone)
* Syndrome Pierre-Marie and Foix (hypertrophic osteoarthropathy pneumiante) with clubbing, inflammatory arthralgia and periosteal apposition on the shaft of long bones; trophic vasomotor disorders.
G- Investigations:
* X-ray: typical proximal perihilar opacity with hilar lymph node, latérotrachéale
* Required Fibroscopy bronchial biopsies with lesions, aspiration cytology. Usually shows extensive infiltration with extrinsic compression proximal aspect. Biopsies may be falsely negative (submucosal tumor development).
* If negative histology -> quickly realize according to radio-clinical data transparietal aspiration biopsies, mediastinoscopy …
* Assessment of extension: endoscopy, chest CT, CT of the head, abdominal ultrasound, bone scan (systematic even in the absence of clinical signs); CT centered on the adrenal; bone marrow biopsy
* Biology: serum electrolytes, liver function tests, calcium and phosphate, creatinine quarry, NSE (initial value for the treatment followed) and LDH (reflecting tumor mass).
* Pretreatment assessment: EFR (only when chest radiation therapy is contemplated and in very rare cases extirpable tumors surgically). ECG; Echocardiography (if use of anthracycline); markers (NSE, LDH).
H- Classification:
TNM stage does not apply to this histology
I- Evolution & treatment:
* In untreated control median survival at 2 months for disseminated forms and 3 to 4 used for localized forms
* Under treatment: median survival of 1 and 2 years for localized forms and 8 months to 1 years for disseminated forms.
* Chemotherapy: very chemosensitive tumors
* Radiation therapy: locoregional; prophylactic brain; for pain relief in bone metastases and / or spinal cord compression
* A complete response is defined iconographic way lung cancer (NPC) -> disappearance of any trace of the original injury on CT scan.
You must be logged in to post a comment.