 CLINICAL SIGNS:
CLINICAL SIGNS:
* none.
* or slow pulse unmodified by exercise or fever for high degree block.
* or feeling weak or lipothymia.
* or syncope of Adams-Stokes .
* or signs of left or global heart failure.
* or sudden death.
ETIOLOGY:
* Idiopathic especially in the elderly, congenital.
* after a myocardial infarction (anterior more derogatory than inferior).
* overload or drug poisoning: digitalis, beta-blockers, Isoptin, Cordarone and other negative chronotropes.
* during Prinzmetal’s angina (trinitrine removes the two anomalies).
* Calcified aortic stenosis.
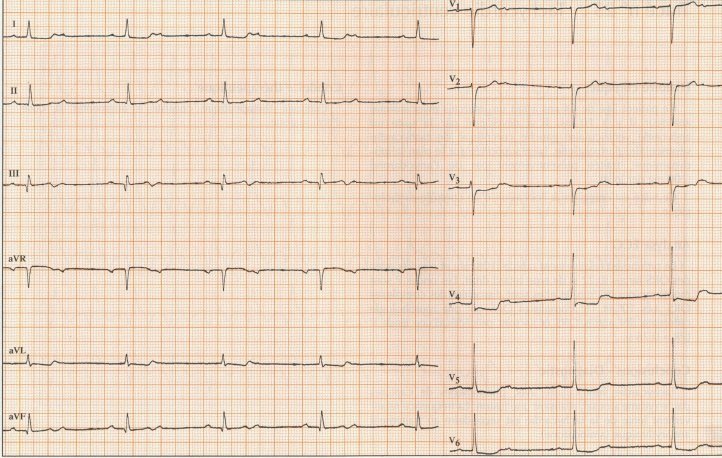
ADDITIONAL TESTS:
* scope, ECG:
– BAV I:
– PR> 0.20 s , asymptomatic.
– BAV II:
– progressive extension of PR until blocking of a P wave not followed by QRS (Luciani-Wenckebach period) or unexpected blocking of the P wave not followed by the QRS wave (Mobitz 2).
– BAV III:
– Complete atrioventricular dissociation , more P waves than the QRS without coupling with them.
– supra-hissian relay (fine QRS), hissian (fine QRS) or infra-hissian (wide QRS).
– presumption of paroxystic complete BAV:
– if BBD + HBPG or BBD + HBAG, BAV II, BBD complete isolated, …
* blood ionogram: look for hypokalemia.
TREATMENT:
* respect a well tolerated bradycardia, stop any negative chronotropic drug.
* if bad tolerance:
– hospitalization.
– venous route: G5%, oxygen therapy in the mask.
– Atropine sulphate: 0.5-1 mg IV, renewable after 5 minutes (maximum 5 mg) but not very effective for the most symptomatic large QRS BAVs.
– if failure or if QT long:
– Isuprel : 5 ampoules in 250 ml to adjust according to the frequency, to maintain above 80 / min (electric syringe in children: 0.1-1 μg / kg / min).
– set up an electrostimulation probe as soon as possible, especially if digitalis intoxication because Isuprel is contraindicated.
* treatment of the cause.