 History of the disease:
History of the disease:
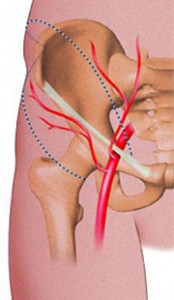
In the early 1980s, several publications reported observations of functional impairment of exercise in high-level cyclists in relation to a first-centimeter stenosis of the external iliac artery. These athletes saw their stress thigh pain appearing at maximum or supra-maximal effort. The arterial origin of the pain was confirmed by the total disappearance of the functional signs after vascular surgery.
Definition:
Histological analysis of the surgical specimens in these patients, most often free of the traditional risk factors for atherosclerosis, revealed an intramolecular fibrous infiltrate of the arterial wall (2). Most lesions sit on the external iliac and appear in the athlete of high level, but nonilial localizations in non-cyclists endurance athletes have now been well documented. Despite a publication challenging the histological aspect of the disease, the term “endofibrosis” seems to be preserved, as well as the “induced exercise” of the disease.
Prevalence:
The actual prevalence of the disease remains poorly understood. It would be close to 30% in some high-level teams and the increase in cases diagnosed in recent years reflects a better knowledge of the disease by physicians and the sporting environment than an increase in the annual incidence of new sportsmen.
Indeed, observations of endofibroses in former sports professionals suggest that the disease was certainly undiagnosed several decades ago.
The prevalences which could be reported in foreign journals should probably not be taken into account, since the definition proposed by some authors, in particular Dutch authors, incorporates stenosive lesions with parietal overload in the diseases of the professional cyclist non-stenosing lesions, only related to arterial stretching. For our part, we retained only pathological patients with significant stenosing lesions, with histological image confirming arterial wall fibrosis.
Physical examination:
In the case of endo-fibrosis, it is conventional to observe a worsening of the symptoms during the competition seasons and a regression of the symptoms at the beginning of the following season if the cycling training is stopped.
It is likely that this is only due to the level of performance achieved by the athletes at different times of the year, rather than a gradual evolution of the disease. The clinical symptoms remain relatively typical in the form of a subjective sensation of big thigh or loss of strength of the affected leg, appearing at maximal effort and regressing in a few minutes when stopping the effort.
Additional tests:
Ultrasound imaging and Doppler are widely used in the diagnosis of vascular diseases and have shown some utility in endofibrosis. However, the predictive value of ultrasound remains modest, and although some observations show velocity accelerations in the resting iliac Doppler, they probably correspond to highly developed lesions that have become rare since patients consult early.
The measurement of ankle systolic blood pressure indexes is an essential component of the diagnosis of endo-fibrosis, as is the case with peripheral arterial disease, although the normality values of athletes are different from those of untrained subjects. Efforts must also be made to ensure that the level of effort provided in the laboratory matches the athlete’s usual performance level, otherwise pain is not replicated and examination may remain negative, falls of the pressure indexes at the ankles depend on the level of load on the cyclo-ergometer.
Numerous threshold values have been proposed in the literature concerning the diagnosis of endofibroses.
It is interesting to note that to the extent that the Dutch teams integrate patients with objective strictures into their patients, but also patients with only elongated and flexed arteries, it is not surprising that the diagnostic value of ankle pressure is low in their group.
It is also interesting to note that although the measurements taking into account the differences in blood pressure on one side compared to the other may have a high diagnostic performance, they may be taken in patients with bilateral lesions, even if they have only unilateral symptoms.
Whatever criteria may be chosen, it seems important to respect some essential points to the measurements of stress pressure index to diagnose endofibroses:
1. the test must always be carried out on a highly trained subject and not after a period of rest;
2. the level of effort provided must be the level of effort that reproduces the symptoms, which requires having an ergometer with high loads in the laboratory;
3. if the stress test does not reproduce the usual symptomatology, the risk of false negative pressure indexes can not be excluded;
4. the earlier the ankle pressure measurement after stopping the stress, the higher the test performance will be;
5. If one is interested in the differences in pressure between the healthy side and the pathological side, it is preferable to have perfectly synchronous measurements either by performing measurements by several operators or by using automatic tensiometers;
6. Measurements should always be carried out in the strictly dorsal position, since if they are made in a sitting position, the ankle pressures are overestimated (roughly a value corresponding to the hydrostatic pressure of the trunk blood column, head and neck).
The magnetic resonance imaging proposed by the Dutch authors is probably relevant and efficient in diagnosing arterial stretching, but does not, in our opinion, fit within the diagnostic logic of fixed arterial stenoses. On the other hand, after the non-invasive examinations, if an arteriography is performed, it seems preferable that it should be done by hands very experienced in this disease, because it is not exceptional, for lack of experience , that the examinations are interpreted as normal, although radiologically minor lesions are present.
The arteriography of the suspect axis should ideally be performed in thigh flexion, so as to see appear plicatures or areas of shrinkage which are sometimes difficult to see on the cliché stretched leg.
Examinations for the future:
With a better knowledge of the disease, the number of extreme-age subjects, as well as foot pedicures addressed for suspicion of endofibrosis, is constantly increasing. It is currently difficult to say whether the diagnostic limits proposed in the literature for cyclists are applicable to other sports. If new techniques were to be developed, perhaps transcutaneous oxygen measurements will provide, as in other vascular situations, a diagnostic element.
Near-infrared near-infrared spectroscopy, which is supposed to measure the saturation of the deep muscles, may be a determining factor in future diagnosis. Finally, thallium scintigraphy, proposed in the diagnosis of proximal ischemia, could be useful for discriminating healthy patients from diseased patients and its diagnostic performance should be studied in the future.
Numerous publications have been made on endofibrosis in the last 20 years (3, 4, 8), but much remains to be learned in the near future about the diagnosis, treatment and pathophysiology of the disease.