MRI is currently the gold standard for morphological study of the hypothalamic-pituitary region, having supplanted the pituitary scanner and X-ray of the sella.
I. INDICATIONS AND CONTRAINDICATIONS:
I.1 information:
Pituitary MRI may have several indications
– A diagnostic purposes: search for a pituitary disease before a tumor mass syndrome (signs of intracranial hypertension with headache, nausea, vomiting) or to an alteration of evocative visual field of a chiasma reached.Search for a hypothalamic-pituitary disease to diabetes insipidus (lesion in the posterior pituitary, craniopharyngioma?)
– A referred prognosis: To assess the degree of local invasion of a hypothalamic tumor (extension to the cavernous sinus chiasma compression, erosion sellar floor)
– As part of the monitoring of a pathology treated The residual tumor after surgery, tumor cast as anti-secretory therapy.
I.2. Cons-indications:
The main cons-indications related to the magnetic field of the device: pacemakers, ferromagnetic cerebral clips, metal chips intraocular, heart valves (except for some newer models). These cons-indications should lead to the practice of a brain scan centered on the pituitary gland with reconstructions. The cons-indication is the existence of severe claustrophobia. The contrast medium injection should be avoided during the first trimester of pregnancy.
II. TECHNIQUE:
The various anatomical components of the hypothalamic pituitary region can be displayed on three types of sections (figure 1):
– Images coronal give an overall indication of the pituitary region and minimize the effects of partial volume induced by adjacent anatomical structures (Figure 2).
– Images sagittal allow the study of the midline structures, especially the posterior pituitary (Figure 3).
– Axial sectional images allow the evaluation of the posterior pituitary, the degree of posterior involvement (brainstem) and anterior (optic chiasm) (Figure 4).
Weighted sequences T1 and T2 may be coupled to the injection of a contrast produced, gadolinium. Remember, water is hypointense on T1 and hyperintense on T2. Aspects sequence T1 and T2 of each major element of the anatomical hypothalamic pituitary region are provided in Table 1.
III. TRAPS AND ANATOMICAL VARIATIONS:
III.1. Anatomic variants:
The main pituitary anatomical variant is related to its maximum height (normal 8 to 9 mm), varies according to age, sex and physiological conditions (pregnancy, Figure 5). The posterior pituitary may be ectopic in healthy subjects or in connection with diseases of pituitary development; the signal intensity is also absent in healthy adults 10 to 20% of cases.
Another anatomical variant relates to the path of the internal carotid arteries (unilateral or bilateral prolapse, which can project into the lodge) which may have an impact on the indication for surgery.
III.2. Traps:
Partial volume: The degree of slice thickness can appear in the same plane two teams that are not.
Magnetic susceptibility artifact: the magnetization capacity is different in different tissues may give false images (eg artifact at the insertion of a wall of the sphenoid sinus may be falsely suggest a pituitary microadenomas).
Pituitary incidentalomas: This is micro images or macroadenomas viewed on brain MRI performed for non-pituitary pattern. It must lead to make a hormonal balance in search of hypo or hyper, support varies depending on the results of this review and the degree of possible invasion of adjacent structures. The high resolution of MRI requires that any imaging examination is justified by prior hormonal balance sheet subject to process images instead of pathologies.
IV. THE RESULTS:
IV.1. Pituitary adenoma:
Before a suspected pituitary adenoma should routinely seek evocative elements of the diagnosis, and then specify the elements essential to the realization of a surgical procedure adapted:
IV.1.A Search pituitary adenoma:
Typical MRI signal: Conventionally, pituitary adenomas have an iso or hypointense signal on T1, hyperintense on T2 Iso or slightly enhanced after contrast injection (hypointense relative to the rest of the pituitary gland). Indirect signs can also provide information on the location of the adenoma: deviation of the pituitary stalk, irregular sellar floor.
The height of the pituitary adenomas microadenomas are defined by a maximum height of less than 1 cm (Figure 1). In contrast, macro-adenomas are defined by more than 1 cm height (Figure 2).
Prolactinomas are typically rather microadenomas except in man (late onset). Cushing’s disease adenomas are more responsible microadenomas, instead of acromegaly, where macro-adenomas invading the cavernous sinus.Generally, for secreting adenomas, the size of macroadenomas is correlated with the degree of hormonal activity (valid especially for prolactinomas).
Appearance changes adenoma
– Hemorrhagic Transformation: Early isointense signal on T1 and T2; and hyperintense signal on T1; can display a horizontal level (sediment deposition) with hypointense signal on T1 and T2 remotely. Is the vector of changes in imaging Sheehan syndrome.
– Tumor Necrosis: hypointense signal on T1 and hyperintense on T2
– Kystisation: it will be viewable in MRI by fluid consistency of image (T1 hypointense on T2, identical in appearance to CSF) within the adenoma.
– Arachnoidocele: final stage of evolution of hemorrhagic necrosis of an adenoma, it is defined as an empty saddle, healthy pituitary gland usually being compressed to the sellar floor.
IV, 1.B Search the complications of pituitary macroadenomas:
If macroadenomas compression, it is often possible to see the healthy pituitary pent growing laterally, with a T1 hypointense relative to healthy pituitary (compared to adenoma), very enhanced after contrast injection.
Evaluate the extension of macroadenomas:
– Infra-sellar: bone deformities of the sellar floor, invasion of the sphenoid sinus
– Suprasellar: chiasmatic compression, compression of the 3rd ventricle and signs of hydrocephalus
– Latero-sellar: the invasion of the cavernous sinus is often difficult to define. According to studies, it is considered in the case of certain higher recovery to half the cavernous sinus or encompassment of more than half of the carotid.
IV.1.C. Specify the data needed for the surgery:
We must seek
– The existence of a collar between the intra-sellar and suprasellar expansion macroadenomas.
This collar can be a cons-indication for vaginal surgery (risk of persistent suprasellar residue).
– The degree of pneumatization of the sphenoid sinus (passageway when first transsphénoïdal) must be specified because it can be a cons-indication for this surgery.
– Prolapse of carotid artery in the cavernous sinus which may be an indication-cons to surgery and to prefer the continuation of an anti-secretory medical treatment or radiotherapy.
– The existence of which does not arachnoidocele against-indicated surgery provided a good view of the adenoma on imaging, but allows to consider the risk of fistula intraoperatively or postoperatively, which can result in a risk of infection (meningitis).
IV.1.D. Monitoring of treatment:
If surgical treatment, post-surgical revisions make it difficult immediate assessment of treatment. The first MRI should be performed 6 months after surgery and will search for any residue or recurrence.
In case of medical treatment, pituitary MRI should be repeated at regular intervals (especially in early treatment initiation) and in the presence of a macroprolactinoma touching the chiasm, MRI should be performed within 10 days after initiation of dopaminergic therapy: in the absence of iron tumor, surgical treatment should be offered.
IV.1.E. Differential diagnosis of pituitary adenomas:
Craniopharyngiomas (see IV.2)
Cysts Rathke’s pouch: secondary residue embryological formation of the pituitary gland, they can cause a moderate hyperprolactinemia by stem disconnection syndrome. They are typically in the sella, in median position in axial section, between the ante and post-pituitary. Because of their mucoid their MRI signal is variable, usually not enhanced after contrast injection.
Arachnoid cyst: developed forward, they typically repress the anterior pituitary backwards and downwards. They have a purely cystic consistency with the same signal on T1 and T2 to the CSF.
Meningioma: they have a suprasellar development, but can suppress the pituitary healthy against the sellar floor.The diagnosis is made on a hyperintense signal on T2 as the anterior pituitary with a very marked contrast enhancement.
Hypophysitis: diffuse inflammation of the pituitary gland by lymphocytic infiltrates in peri-partum context. The pituitary is conventionally increased symmetrically volume, with a strong homogeneous contrast enhancement.
Pituitary abscess: usually secondary to sphenoid sinusitis or iatrogenic after surgery, they are recognizable by their necrotic center hypo- or isointense or hyperintense T1 and T2 iso, surrounded by a thick shell taking strong contrast.
IV.2 Craniopharyngioma:
It is a benign epithelial tumor developed in the sellar suprasellar region.
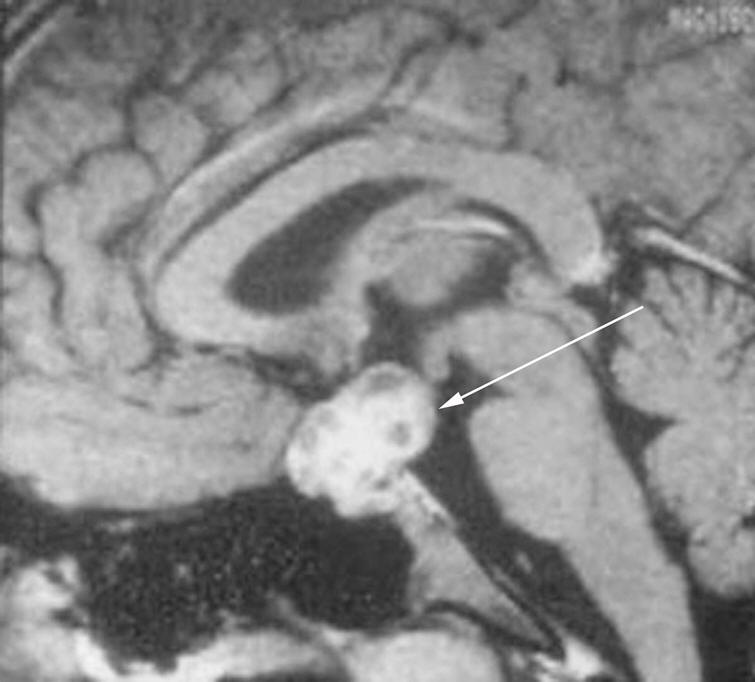
Conventionally, the craniopharyngioma combines three quotas (Figure 8):
– A tissue contingent, mixed and fleshy heterogeneous composition rather isointense signal to the pituitary, enhanced by the contrast medium injection
– A quota cystic fluid component (T1 hypointense identical to CSF) and / or protein (hyperintense T1) not enhanced
– Calcifications (hypointense T1 and T2 MRI) better visualized by a scanner, ring or nodular.
The three quotas are not always present, one can observe purely cystic craniopharyngiomas or tissue. The enhancement is usually wall or ring.
Before an MRI suggestive of craniopharyngioma you have to specify
– The volume of the lesion
– The seat of the lesion: intra infra and supra-sellar
– The different quotas (impact during surgery)
– The degree of extension (chiasm, pituitary stalk, invasion of the third ventricle); craniopharyngiomas typically have suprasellar extension rétrochiasmatique, driving healthy pituitary down.
Main pitfall to avoid: Do not confuse the calcification of craniopharyngioma with parietal calcifications of an aneurysm. If in doubt, an MRI angiography should be performed.
IV.3 Diseases of the pituitary stalk and posterior pituitary:
Some systemic inflammatory diseases (histiocytosis X, sarcoidosis) have an impact on the central nervous system, particularly the hypothalamic region.
These inflammatory conditions will result in a loss of MRI hyperintensity of the posterior pituitary (presence of diabetes insipidus in review) sometimes associated with hypertrophy of the pituitary stalk (isointense T1 and T2 enhanced homogeneously after contrast, Figure 9). Neurosarcoidosis also associates the presence of sarcoid granules that can infiltrate the floor of the third ventricle heterogeneously enhanced after contrast.
TB can also be the cause of an enlarged pituitary stalk with dissemination tuberculoma with contrast “ring”.












Leave a Reply