* The non-Q wave infarction: IDM Nontransmural, has no Q-wave Contains intense as ST depression or T wave ischemia (sustainable). With increase in cardiac enzymes.
Timeline & morphology:
In the March 1 H:
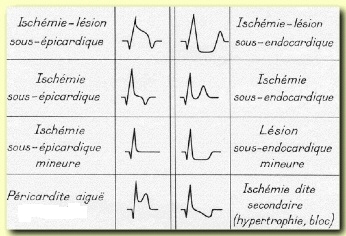
Giant waves symmetrical T (subendocardial ischemia)
By the fourth hour:
STEMI ST convex upwards encompassing the T wave -> is the wave Pardee signing the sub-pericardial injury
By the sixth hour:
Q wave of necrosis (> 0.04 s); it reaches its peak to 12 hours
Then:
Shift-addition to the regression of ST segment (in 2-3 weeks) with negativity of the T wave to the 2nd or 3rd day
* Note: the offset-plus persistence ST beyond the 3rd week (or 4th week) should be suspected aneurysm post-MI LV
* The left bundle branch block (LBBB) mask the signs of anterior infarction (QS aspect V1-V3); the sign of Cabrera is a hooking the bottom portion of the S wave directed towards the diagnosis of MI in the event of BBG.
Location:
Q wave in V1-V2-V3 -> Myocardial anterior septal
Q wave in V1-V2-V3-V4 -> Myocardial anterior septo-apical
Q wave in V1 to V6 D1 + and V -> extensive anterior infarct
Q wave in V4 -> apical infarction (with microvoltage in the limb leads
Q waves in D2-D3-VF -> lower Infarction
Q wave in V5-V6 -> Lateral Infarction
Q waves in D1-VL -> top lateral infarction
Q wave in D2-D3-VF + V1-V2-V3 -> Myocardial deep septal
Q wave in D2-D3-D3 + D1 + VL-V5-V6 -> Lateral Myocardial infero-
Q wave in V7-V8-V9 + mirror (R V1) -> basal Infarction
Q wave in D2-D3-VF and V7-V8-V9 -> Myocardial infero- basal
* The prior IDM meets with impaired left coronary (anterior interventricular)
* The bottom or side IDM -> right or circumflex coronary artery disease.
* Recurrence in the opposite territory may cancel the first signs of IDM (IDM recent previous Q wave that clears the bottom of an old MI)

Leave a Reply