* TOXOPLASMA EYE: relapsing chorioretinitis; hyalite. Manifested by myodésopsies and decreased visual acuity. In FO, whitish home that progresses to atrophic scar
1- Multiple sclerosis:
A- Neuropathy:
* Visual acuity (-); retrobulbar pain; Direct RPM (-)
* Review the fundus is normal (retrobulbar neuropathy)
* Visual Fields: central scotoma or COECO-central
* Uhthoff’s phenomenon: thermolability of demyelinated axons
B- Achievement oculomotor:
* VI palsy
* Internuclear ophthalmoplegia (very evocative)

2- hypertension:
A- RETINOPATHY HYPERTENSIVE:
– The first sign is the decrease in arterial caliber (vasoconstriction)
– Retinal hemorrhages splinter
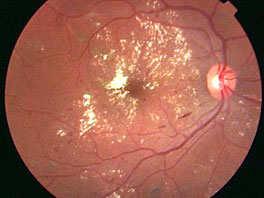
– Macular edema associated with dry exudate (deep) which reflects the sustainable disruption of the blood-retinal barrier (OHR) -> stellar available (macular star)
– Papilledema (-> enlargement of the blind spot)
– Nodules cottony (arteriolar occlusion) regresses after treatment of hypertension
– Deep retinal hemorrhage (occlusion of arterioles -> retinal infarction)
– The decrease in visual acuity is rare
B- choroidopathy HYPERTENSIVE:
– Ischemia and necrosis of the pigment epithelium by choriocapillaris occlusion
– Acute phase -> Elschnig spot (small deep pigmented spots)
– Exudative retinal detachment in the posterior pole
C- ARTERIOSCLEROSIS:
– Enhancement reflection arteriolar the eye of background due to wall thickening
– Crossing Sign (retinal vein is overwritten by the dilated artery and upstream)
– Préthrombose -> retinal hemorrhage at the intersection worthy
– Retinal Vein Occlusion
D- CLASSIFICATION:
* Stage I: frozen arteries brilliant
* Stage II: crossing sign
* Stage III: retinal hemorrhages and cotton wool spots; venous dilatation
* Stage IV: papilledema
3- Diabetes:
* The edematous phenomena predominate in the macula; occlusive phenomena affect primarily the peripheral retina (ischemia -> neovascularization)
* The hard exudates are secondary to the precipitation of plasma lipoproteins in the thickness of the retina; are usually arranged in a ring (exudates circinate)
* Intra-retinal microvascular abnormalities (IRMA) and dilation telangiectasia Vasc
* Non priliférante retinopathy: puncture intra-retinal hemorrhages, microaneurysms, hard exudates, cystoid macular edema (WTO) or not; cotton wool spots
* R. preproliferative: irregular dilated veins “rosary”; peripheral ischemia; significant intra-retinal hemorrhages; AMIR
* R. proliferative: new vessels; rubeosis iridis (iris neovascularization)
* Complications R. proliferative: HIV (neo-vx prépapillaires) glaucoma (rubeosis iridis) retinal detachment by traction (neo-vx prépapillaires)
* Other complications maculopathies (edema, ischemia)
* Causes of blindness: macular edema (cystoid or not); ischemic maculopathy; exudates central foveal dry; retinal detachment; glaucoma.
* Angiography is indicated when there is a R & D FO and is not routine in any diabetic; it specifies better the extent of retinal ischemia and time of the laser.
* The laser panretinal photocoagulation is the specific treatment of proliferative R.. The treatment should be urgent in appearance of new vessels Preretinal.
* Laser treatment of maculopathy: indicated in cases of edema if there is a (-) of the significant and prolonged visual acuity; in case of hard exudates; TRT is not urgent.
4- Other complications:
* Infectious: stye relapsed; blepharitis; dacryocystitis
* Lens: Cataract; early presbyopia
* Oculomotor paralysis
Leave a Reply