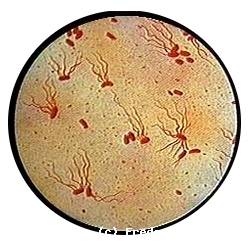
* This is a septicemic poisoning (S. enterica / Typhi) at the point of departure mesenteric lymph caused by the bacillus of Eberth.
The germ of the reservoir is represented by the man.
* S. Typhi and Paratyphi The C can carry said Vi capsular Ag (used in the vaccination).
Facultative intracellular bacterium.
* The onset is usually gradual; the temperature rises steadily to reach 40 ° C in a week. Epistaxis is a classic but inconstant sign.
Frontal headaches, insomnia, fatigue, anorexia, abdominal pain, constipation.
* The beginning can be brutal, picture gastroenteritis or appendicitis (child).

* Status phase: the fever keeps tray (39-40 ° C); drowsiness, confusion way (typhoid state) with nocturnal insomnia and abdominal pain.
Diarrhea “melon juice”; the pulse is separated, the language is saburral, Duguet angina (10%); FID gurgling; the abdomen is sensitive.
Splenomegaly.
Pink spots lenticular (1/3 of cases).
* Orientation Review: VS be high and low CRP also.Leukoneutropenia (leukocytosis may be in the child).
Sometimes thrombocytopenia. Elevated transaminases …
* Blood cultures (or myélocultures) are positive especially during the first week.
Stool cultures were positive in 40% of cases after the 10th day.
* Serology Widal-Felix: it contributes little to the diagnosis.
It becomes posi-tive from the 8th day. Anti-O Ac disappear within 2 to 3 months; Anti-H persis-tent for years.
But serology may be falsely positive in Yersinia infection, typhoid, malaria, minor salmonellosis, dysglobulinemia.
* Digestive Complications: lower GI bleeding; perforation with peritonitis.
* Complications toxin: neurological (encephalitis); heart (myocarditis); pseudo-of perforation syndrome (cause: phenicols in high doses).
* Bacterial Dissemination: cholecystitis; osteitis; splenic abscess …
* Classic Treatment: phenicols; amoxicillin; cotrimoxazole.
The duration is 2 weeks. (In Algeria -> thiamphenicol for 21 days)
* Treatment for adults (in Europe): fluoroquinolone for 7 days.
In children using ceftriaxone for 5 days.
* Corticosteroid therapy is reserved for cases where the signs are major toxin.
* Note: in the pseudo-of perforation syndrome (which is toxin mechanism -> paralytic ileus) NSF shows neutropenia (leukocytosis in true perforations) treatment consists of corticosteroid therapy.
* Monitoring: Control blood count; ECG; at the end of the treatment two stool cultures are made 48 hours apart.
* Typhoid is not an immunizing disease; vaccination is possible (Ag Vi)
Leave a Reply